 ENG
ENG






INTRODUCTION
Obtaining precison and passive fit of the restorations has always been the greatest challenge in cases supported by 3 or more implants.
Over the years, numerous impression techniques have been recommended. The most widespread and well documented for full-arch rehabilitations is using pick-up transfer and impression plaster.
Recently, the improvements made to intraoral scanners (IOS) have aroused growing interest in the application of optical impression techniques to more complex/advanced cases. The precision and accuracy of IOS in detecting single-element and quadrant restorations is now consolidated practice. Problems still exist in taking impressions of complete arches, even more when the restorations are supported by osseointegrated implants which are solid with the bone: they do not allow large misfits of the superstructures to be compensated for, especially in the case of screw-retained restorations.
In recent years, photogrammetry techniques have been introduced and applied to the detection of full-arch impressions on implants. The available scanners have some noteworthy limitations: the scan is extraoral, it is therefore necessary to use “surgical” retractors/mouth openers which are poorly tolerated by patients in the absence of anesthesia; the scanners are bulky and quite heavy, therefore they must be manipulated with two hands, holding them like a camera; the cost of these devices is high and their use is limited to taking the impression of the position of implants: they must be integrated with a “standard” IOS to take impressions of the mucosa of the edentulous arch, of the opposing dentition and the registration of the intermaxillary relationship.
A few weeks ago, the first (and to date only) intraoral photogrammetric scanner (IPG) was intoduced (Aoralscan Elite, Shining 3D Dental). This device combines a standard IOS with a photogrammetric scanner. With a single device, it is therefore possible to capture the classic intraoral scans for simple restorations on natural teeth and implants, as well as the relative position of implants for screw-retained restorations. Preliminary data on the accuracy of implant scanning have confirmed tolerances within 5 µm (manufacturer data).
Two clinical cases of full-arch implant rehabilitations will be shown below. Both were treated with a full-digital protocol, which includes:
- Optical impressions of the arches and the intermaxillary relationship using an IOS.
- Capture of the implant positions with IPG.
- Milling of the fixed prosthesis with a 5-axis milling machine.
- Cementation of the ti-bases “in hand”, without the use of stereolithographic models.
- Verification of the impression accuracy. Using photogrammetric data, an oversized metal bar was designed, milled and intraorally tested for accuracy and fit.
CASE 1
79-year-old woman with only teeth 21 and 22 remaining in the upper arch. Negative medical history for systemic diseases, marked claustrophobia, and moderate gag reflex.
Four implants were planned to rehabilitate the edentulous arch opting for a protocol with angled implants to utilize the available bone.
After inserting the implants, angled abutments were selected and placed on the implants, 30° on the distal implants and 17° on the anterior ones.
Impressions of the arches and the intermaxillary relationship were captured, followed by the intraoral photogrammetry of the implants (Pic. 1). Based on the captured data, a monolithic PMMA arch was fabricated and screw-retained on the implants. The time interval between the end of surgery and the delivery of the immediate-load provisional prosthesis was 24 hours (Pic. 2).


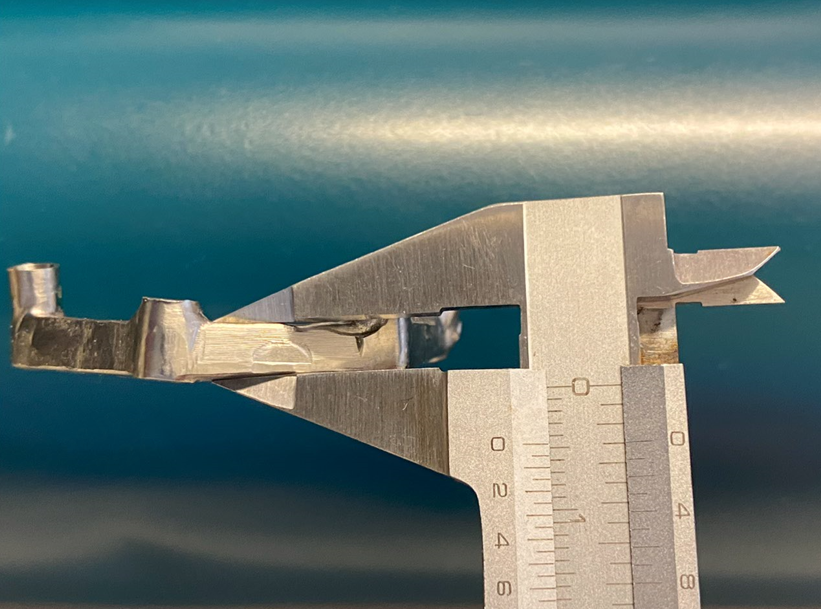
A square-section bar of 4.5 mm per side was designed based on the intraoral scan data (Fig. 3) and milled from a cobalt-chrome disc.
One week after surgery, when sutures were removed, the temporary prosthesis was also removed, and the metal bar was tested by performing the one-screw “Sheffield test”: the bar was screwed at one end, an intraoral x-ray was taken at the implant at the opposite end of the bar. The test was repeated switching sides. (Pics. 4-6).


Fig 5 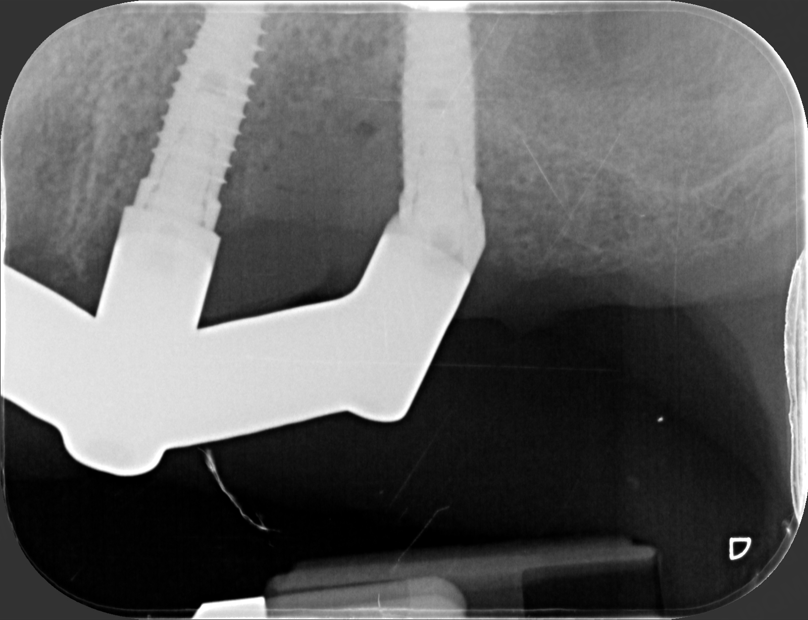
Fig 6
CASE 2
66-year-old woman presents with terminal dentition due to caries under previous restorations and advanced periodontal lesions. The patient had early-stage type II diabetes controlled with oral therapy and smoked approximately 10 cigarettes/day.
Due to anatomical conditions and concomitant diseases, a staged approach was opted for. Teeth were extracted, bone and mucosa were left to heal for two months. Implants were placed together with bone grafts in areas of dehiscence. The patient wore a complete denture during this phase. After four months of healing phase-two surgery was performed, four abutments were connected to the implants, and intraoral impressions were taken, as in the previous case (Pic. 7).

The prosthesis was also delivered 24 hours after surgery (Pic. 8), and after one week the titanium bar was tested with the “Sheffield test” (Pics. 9-11).


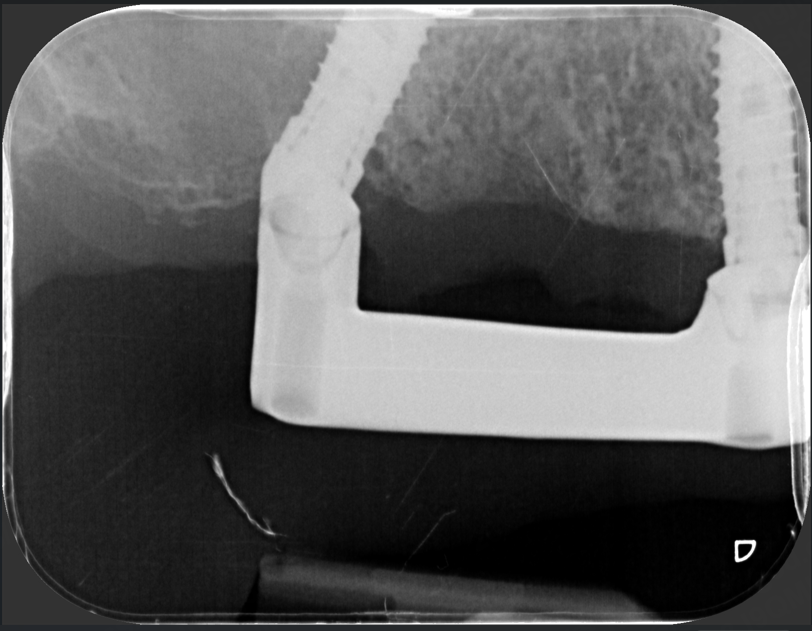
Fig 10 
Fig 11
Due to its greater radiolucency, titanium allows for even better assessment of the bar’s fit on the angled abutments.
DISCUSSION
This protocol allowed, in the presented cases, to obtain passive fitting prostheses within an amount of time similar to a standard intraoral scan. The scanner is small, lightweight, and handy even when dealing with limited space scenarios.
The scan flags (scan bodies for photogrammetry) are only apparently bulky: both patients tolerated the procedure well and were surprised by the absence of traditional impression materials.
The precision and accuracy of the impressions were verified radiographically, not only with the provisional prostheses but also by fabricating oversized metal bars. This choice was made to eliminate any doubt of false positive passivity due to the elasticity of monolithic PMMA structures. Metal bars, due to their size and material properties, have minimal flexion, so their passive fit is sufficient proof of the impression’s reliability.
These results appear consistent with the most recent reviews of the literature that, comparing “traditional” plaster impressions, intraoral scans and photogrammetry, have found photogrammetry offered superior precision and accuracy compared to traditional impressions.
With the limitations related to the small number of cases treated, this technique proves to be reliable and with predictable results.
Written by:

Doct. Marco Iorio DDS; Private practice in Castelletto Ticino (NO) Italy; limited to fixed prosthodontics, oral and implant surgery; Active member of Italian Academy of Osseointegration (IAO)

Dental technician, laboratory owner with offices in Lombardy and Piedmont, Exocad Biomax trainer
REFERENCES (References are listed in the document but omitted here for brevity.)