 ENG
ENG







Introduction and Patient Presentation
A patient presented with mobile dental bridges, significant difficulty chewing, and dissatisfaction with their overall dental esthetics. A preliminary assessment involved panoramic X-rays and intraoral scanning to evaluate dental status, bone quality, and available prosthetic space.




After thorough diagnostics, a bilateral All-on-X treatment was selected to comprehensively rehabilitate both maxillary and mandibular arches.
comprehensively rehabilitate both maxillary and mandibular arches.
Diagnostic Planning
Cone Beam Computed Tomography (CBCT) scans were acquired for both the maxillary and mandibular arches. These scans provided critical insights into available bone volume, bone density, and anatomical considerations, forming a foundation for precise implant planning and guided surgery.

On the upper arch, for proper placement of implants, extractions with grafting were performed.


On the lower arch, a bone defect was present in the vicinity of the mental foramen and patient recalled having a multiple apicectomy performed in the past that, together with the lack of bone in the distal part of the left mandible, also needed the extraction protocols be implemented together with GBR procedures on the said defects.
Pre implant placement preparations
Since the surgeries took place on different appointments we decided to create interim dentures for the patient after each surgery, with the disadvantage that this flow of events would have to maintain the tilted position of the occlusal plane for the time being. For this to happen a scan of the previously operated jaw was performed.


This tray was used for border molding and analog impression and then scanned with a lab scanner as seen in the next photo.
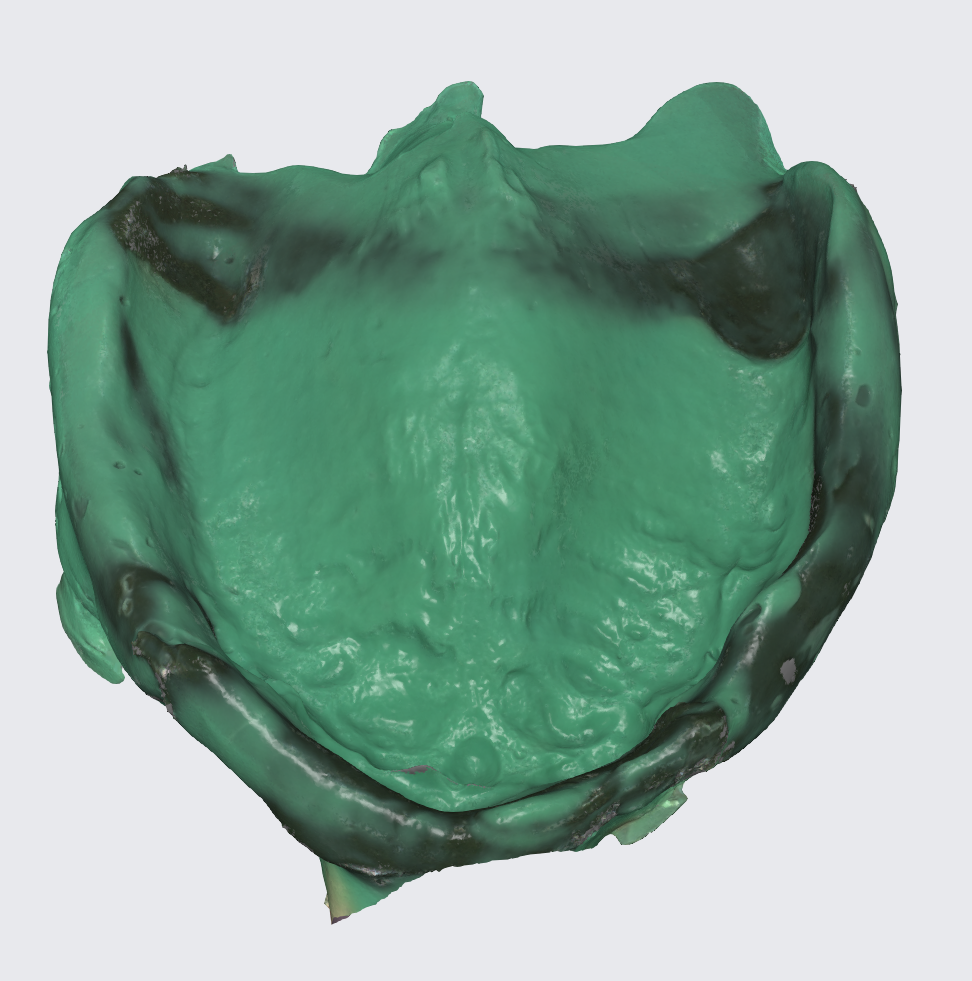


After the same procedure was performed on the mandible a new set of dentures with corrected occlusal plane was produced and we waited for approximately 6 months that passed with uneventful healing.
Advanced Digital Workflow Integration
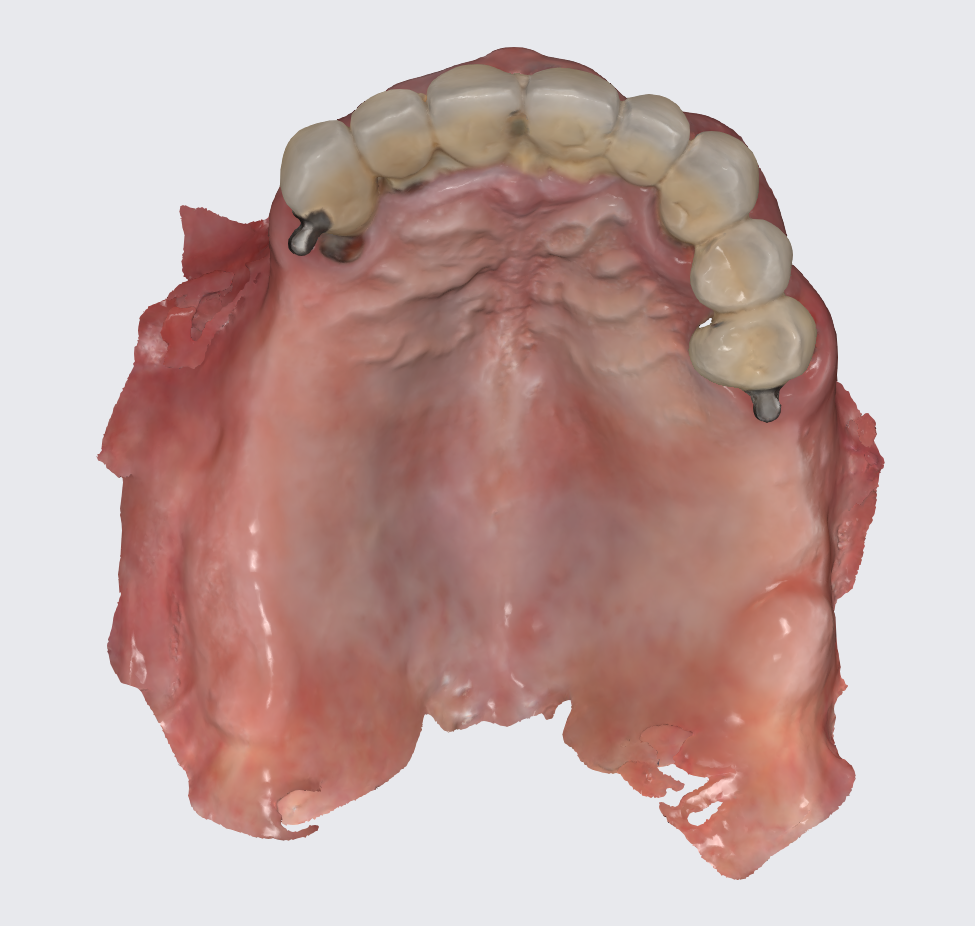
To prepare for the maxillary all on X procedure patient had the upper denture relined with impression material and also multiple dots of radio opaque filling material where temporarily placed on the said denture. Then the 2 dentures where scanned. Also scans of the healed tissues and of the face where recorded.



Using the Aoralscan Elite intraoral scanner (Shining 3D), detailed scans of edentulous ridges and interim prostheses were recorded efficiently and accurately. Edentulous arch scanning proved precise and rapid, significantly simplifying the workflow.

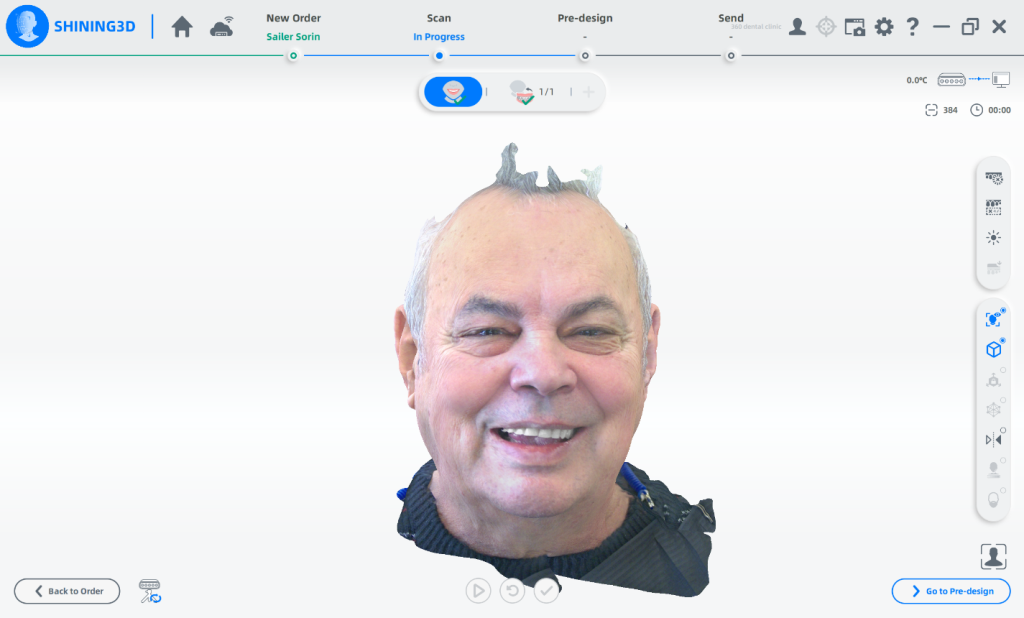
Shining 3D Metismile face scanner was used to perform the face scan and also alignment of intra oral data with the said face mesh. With the new updates teeth color is corrected on the intra oral scan to match the one recorded by the Metismile so that a more coherent look can be generated. Lip contour was automatically removed from the face scan after data matching.
Patient had a new maxillary CT performed with the 2 dentures in occlusion.

Bone was measured to asses the amount of bone gained and the density of the said bone and also a first simulation of implant placement was performed.

Another view of the post graft healing in the mandibular arch and visibility of the composite marker additions done on the upper denture for alignment purposes between scan image and CBCT datasets.
A new waxup was generated in Exocad and printed as a try in to check occlusion but also esthetics at some degree and have a proprosthetic implant positioning available in the planning step.



Surgical and Prosthetic Phase
Implant placement planning done in EXOPLAN involved careful digital matching of the CBCT, wax-up, and facial scan data, resulting in an accurate, digitally-produced try-in prosthesis (Fig. 8). The validated prosthetic design was subsequently integrated with the software to plan placement of five strategically positioned implants in the upper arch.




A modified full arch guide was produced that allowed for implant placement with a flapped approach and no tissue punching for preservation of fixed soft tissue and visual verification of maxillary bone.


Guides produced in Exoplan . Irrigation is easily achievable and soft tissue can be repositioned to not get harmed by the burr .
Surgery was performed and after suturing scans of the patient where only performed for the upper arch and this scans where merged to the preoperator projects.
Postoperative Assessment and Immediate Loading
Because of the Aoralscan Elite bloodied arch was very easy to capture and was achieved in under one minute . For implant position the Intra Oral Photogrammetric procedure of this unique scanner was employed . Scan flags should always be visible in sets of at least 2 at a time so the software can estimate the position of one to the other . This scan took only 20 seconds and after processing these particular scan flags where replaced with their library counterparts for the implants and multiunits used for our patient . With a precision of under 20 microns per full arch this in turn will deliver a perfectly passive fit for the temp all on x bridge.


Postop scan of the arch after removal of healing caps so the technician can chose what scan will be freeformed for the temporary bridge.


The scanned arch and implant position will be used to modify the waxup intaglio and cut out screw channels and direct to MUA connections.
For this procedure we chose the ROSEN Screw to be able to print a bridge and to not need to cement TiBases that would introduce and imprecision with every cement gap of every implant connection. Also with this screw a torque of only 10 N ( so basically hand screwed ) is necessary and because of the small space necessary to fit them in the design the walls of the preparation are far thicker then usual and this leads to less breakage in the temps.

After final design was achieved a Temporary bridge was printed out of definitive resin with the help of the Shining Accufab CEL ,then washed in the FabWash , individualized with the candy coat technique and post cured with the FabCure2 and in around one hour and thirty minutes from the scan was then delivered to the patient. This allows for same day All on X delivery.




Results and Discussion
The immediate results of the All-on-X procedure demonstrated a substantial improvement in both function and esthetics. The use of digital tools throughout the workflow—including intraoral scanners, CBCT imaging, Exocad, and Exoplan software—ensured a highly precise and efficient process. The combination of guided surgery and intraoral photogrammetry enabled a passive fit of the provisional prostheses, minimizing stress on implants and soft tissues.
The patient reported significant improvement in chewing ability and overall comfort, with particular appreciation for the immediate restoration. Esthetically, the digitally designed teeth offered enhanced facial harmony, proper lip support, and a natural smile, all of which contributed to a high level of patient satisfaction. Moreover, the use of provisional restorations throughout the healing phase allowed the patient to avoid extended edentulous periods, thus preserving confidence and function during treatment.
The precision of the digital workflow was especially evident during the immediate postoperative phase, where scanning the edentulous and sutured arch was completed rapidly and accurately. The final temporary bridge fit passively and required minimal occlusal adjustment, reflecting the accuracy of data capture and design. This outcome exemplifies the significant clinical value of incorporating advanced intraoral photogrammetry and digital prosthetic planning into full-arch rehabilitation protocols.
Conclusion
This case highlights the effectiveness of a fully digital, staged All-on-X rehabilitation in a patient with failing prostheses and compromised bone anatomy. From diagnosis to final provisional delivery, each phase benefited from an integrated digital workflow—leveraging CBCT, facial scanning, intraoral photogrammetry, and CAD software.
Key outcomes include:
- Accurate implant placement with minimal surgical trauma.
- Immediate function and esthetic improvement through same-day prosthesis delivery.
- Enhanced patient comfort and confidence during and after treatment.
- Streamlined communication between clinical and technical teams.
The combination of modern imaging, digital design, and guided surgical techniques allowed for a predictable and efficient restoration, resulting in a highly functional and esthetically pleasing outcome. This approach serves as a model for comprehensive full-arch implant rehabilitation in complex clinical cases.
Dr. Alexandru Bogdan
Dr. Alexandru Sever Bogdan is a general dentist in Romania, he owns a clinic in Sibiu where
working completely digital for more than 7 years. He is a very experienced Dentist in implants and restorations.
